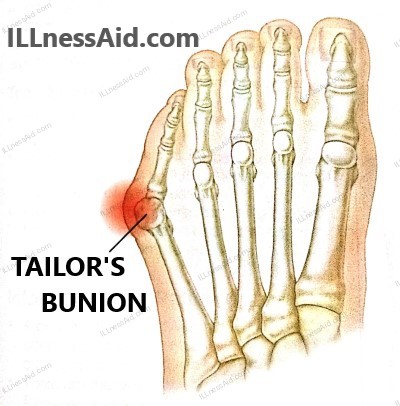
A bunionette, or tailor’s bunion, is a bony protrusion of the fifth metatarsal head that is frequently accompanied by bursitis and corns. This article examines tailor’s bunion’s common causes, patient histories, examination techniques, available treatments, and preventative measures.
INTRODUCTION
A common foot deformity known as tailor’s bunion, or bunionette, is characterized by a bony protrusion on the fifth metatarsal head. Even though it is frequently asymptomatic, problems such as pain and discomfort may arise. Effective management requires an understanding of the condition’s etiology, symptoms, and available treatments.
ICD-10-CM CODE
- M21.62X – TAILOR’S BUNION / BUNIONETTE
CAUSES OF TAILOR’S BUNION
The following are some of the reasons that lead to the tailor’s bunion development:
- Sports: Running long distances or performing other activities that need the foot to be under constant strain.
- Idiopathic: This ailment can happen for no apparent reason and is frequently seen in people who don’t have any obvious triggers.
- Biomechanical Causes: Unbalances or structural irregularities in the foot mechanics might lead to a tailor’s bunion.
- Rheumatoid Arthritis: The likelihood of acquiring tailor’s bunion may be elevated by inflammatory joint disorders such as rheumatoid arthritis.
- Incomplete Intermetatarsal Ligament Development: Problems with the intermetatarsal ligament’s development might result in the development of a bunionette.
HISTORY OF TAILOR’S BUNION PATIENT
Now there are very similar histories for tailor’s bunion patients that we will discuss. So that we can move one step forward to understanding the Tailor’s bunion:
- It is very common abnormality but majorly it is asymptomatic
- Symptoms present from adolescence to middle age
- Pain around the fifth metatarsal head
- Symptoms increase with constructive footwear
- Patients may report a history of corn in the affected area
- History of predisposing features like altered sensation, increased activity, restrictive footwear, etc
- Patients may show a history of skin color changes, swelling, ulceration, etc.
EXAMINATION OF TAILOR’S BUNION
1. PHYSICAL EXAMINATION
A. Observation
- Gait may be disturbed
- Show bony prominence of the fifth metatarsal head
- The size of the protuberance may be increased by the inflammation and hypertrophic bursa
- Observe for predisposing deformities of the foot
B. Palpation
- Tenderness will present directly on the fifth metatarsal head or plantar lateral
- The Head of plantar metatarsal fat may be atrophied in some conditions like diabetes
C. Range of motion
- The fifth metatarsophalangeal joint will subluxate or dislocate
D. Special tests
- Neurovascular examination
- Carefully examination for ulcers and chronic examination
2. IMAGING
- Radiographs examination with the help of X-rays
- Magnetic resonance imaging may be useful
- A dual CT scan may be useful if suspect of gout
TREATMENT FOR TAILOR’S BUNION
1. CONSERVATIVE
- FOOTWEAR: We can use a wide, deep-toe box and semirigid shoes without heels. Padding can also be adjusted for the tailor’s bunion deformity.
- ORTHOSES: We may include hindfoot orthoses(corrective) if the pathology is secondary. Midfoot and forefoot orthoses can also be used.
- CHIROPODY: You should go to good practitioners, That will help you with pain management and symptomatic relief.
- ANTIINFLAMMATORY MEDICATION: Analgesics are mainly used as a first-line treatment. Nonsteroid anti-inflammatory drugs may decrease the duration of exacerbation of inflamed structures (bursa).
2. SURGICAL
For patients in which conservative treatment fails then surgical treatment is the option. It includes head resection, exostectomy, and a variety of metatarsal osteotomies. After the surgery patient may able to fully weight bear in stiff-soled(post-operative shoe) immediately. They have to continue these shoes to wear for 6 weeks(it can vary).
3. EXERCISES
The muscle around the little toe is the “abductor digiti minimi”. This muscle can help reduce the progression of this tailor’s bunion. If you do regular exercise this muscle then it can prevent this deformity and also help in treating the bunion.

Spread your toes softly apart, elevate your foot off the ground, and sit or stand comfortably. Hold for a short while before letting go. Do this exercise ten to fifteen times over.

- Use a theraband/cloth/finger to pull your toe out and up(as in the figure) then press down
- Do these 4-5 lifts several times a day.
Put your foot on a little, soft ball, such as a tennis ball, while you’re seated. Applying light pressure, roll the ball under your foot to work the intrinsic muscles. Focusing on any painful spots, do this for five to ten minutes.

INFORMATION FOR PATIENTS
- A bunionette/tailor’s bunion is relatively common and is often mostly idiopathic but may be associated with other generalized systemic diseases.
- There are many good and successful conservative therapies, you should look for them.
- Mode surgeries have a high chance and are also good, you should believe in doctors. The complication rate depends on the patient’s general health.
THINK, STAND, DO ARE THREE STEPS TO DO ANY WORK
ILLnessAid
Thank you for reading this, today we talk about tailor’s bunion and its treatment, exercises, and more. if you have any doubts regarding this then you can comment below or go to the contact us page.