Alterations in scapular motion and position are known as “Scapular Dyskinesis“. It is present in about 67% to 100% of shoulder injuries. To accomplish most shoulder functions, scapula position and move according to arm motions. The movement of the scapula and humerus is essential for an efficient shoulder function. The scapula plays several roles in shoulder function. It includes control of static position, motions and translations that allow the scapula to these roles.

CAUSES OF SCAPULAR DYSKINESIS
Scapular dyskinesia is a non-specific response to a painful condition in the shoulder rather than a specific response. It has many causative factors like:
- Proximally based
- Muscle weakness/imbalance
- Nerve injury
- Distally based
- AC joint injury
- Superior labral tears
- Rotator cuff injury
The dyskinesia changes the roles of the scapula in the scapular-humeral rhythm. It can be due to alteration in the bony stabilizers, alteration in muscle activation patterns, or strength in the dynamic muscle stabilizers.
Treatment For Scapular Dyskinesis
Treatment of scapular dyskinesis will be successful only when the anatomic base is accurate. The patient assessments should evaluate for problems such as nerve injury or scapular muscle detachment. Similarly, bony or tissue derangement issues such as acromioclavicular separation, fractured clavicle, injury to the labrum, rotator cuff disease, or glenohumeral instability. The large number of cases of scapular dyskinesis are the result of muscle weakness or inflexibility that can be managed with rehabilitation.
Treating Inflexibilities
Inflexible pectoralis minor decreases scapular posterior tilt, upward rotation, and external rotation means scapula movement. If posterior muscles are stiff then there is internal rotation deficit. The sleeper and cross-body adduction stretches can help with the tightness of posterior muscles and soft tissue. Whereas the open book stretch can help in anterior structures.
If there is a capsular stiffness, joint mobilization may be helpful to restore shoulder joint arthrokinematics.
Treating Weakness
A logical progression of from isometric to dynamic exercise focuses on strengthening the lower trapezius and serratus anterior. All of the exercises may be implemented in pre-operative therapy protocol to correct deficits and weakness. However, the dynamic exercises can start in later stages and progress as healing allows.
Once scapular control is achieved, Rotator cuff exercises that stimulate rotator cuff activation are added. Long lever exercises will add during the stage of rehabilitation. Various abduction and flexion exercises will add, with different amounts or types of resistance. Let’s discuss in detail about rehabilitation program.
Rehabilitation Program For Scapular Dyskinesis
Acute Phase (Usually 0-3 Weeks)
- Initially, avoid the painful movement of the arm and establish scapular motion.
- If muscular inflexibility is limiting motion then begin soft tissue mobilization, electrical modalities, ultrasound, and assisted stretching. The pectoralis minor, levator scapulae, upper trapezius, latissimus dorsi, infraspinatus, and teres minor are frequently inflexible due to the injury.
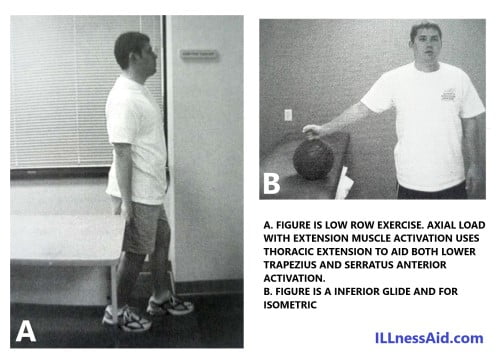
- Use modalities and active, active-assisted, passive, and Proprioceptive neuromuscular facilitation stretching techniques for these areas. To promote safe co-contraction, begin upper extremity weight shifts, wobble board exercises, rhythmic ball stabilization, and low row exercises.
- Use closed kinetic chain exercises in various planes and levels of elevation along with appropriate scapular positioning.
- Initiate scapular motion exercises without elevation of the arm.
- Use trunk flexion and forward rotation to initiate scapular protraction and active trunk extension, backward rotation, and hip extension to initiate scapular retraction. For these postural changes, the patient needs to assume a contralateral side-foot-forward stance and actively shift body weight forward for protraction and backward for retraction. Patients who are unable to do the trunk motion with the hips from this stance may actively stride forward and back with each reciprocal motion.
- Include arm motion with scapular motion exercises because scapular motion improves to re-establish scapulohumeral coupling patterns. Keep the arm close to the body initially to reduce the intrinsic load.
- Do lower abdominal and hip extensor exercises from the standing position. These muscle groups help stabilize the core and in establishing thoracic posture.
Full active scapular motion is limited by muscular inflexibility and myofascial restrictions. These soft tissue limitations should alleviate for successful scapular rehabilitation. The restriction of motion and pain due to these conditions limits progression through rehabilitation and leads to compensation of muscular patterns, impingement, and possible glenohumeral joint injury.
Recovery Phase (3-8 weeks)
Muscular activation and proximal stability are important for appropriate scapular motion and strengthening, Strengthening is dependent on motion, and motion is dependent on posture.
- Should continue to emphasize lower abdominal and hip extensor exercises along with flexibility exercises for the scapular stabilizers.
- Increase the loads on CKC(close kinematic chain) exercises such as wall push-ups, table push-ups, modified prone push-ups, etc.
- Also, increase the level of arm elevation in CKC(close kinematic chain) exercises as scapular control improves.
Position the patient for CKC(close kinematic chain) exercises by placing the hand on a wall, table, or other object and then moving the body relative to the fixed hand to define the plane and degree of elevation. This method confirms the appropriate scapular position relative to the position of the arm. If the normal scapular positioning cannot achieve in this way, the arm position requires adjustment.
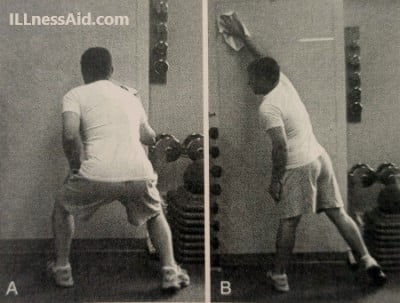
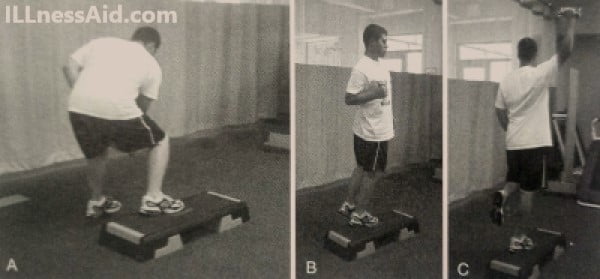
- Use the diagonal patterns, scapular plane, and flexion to help achieve arm elevation. Progress toward the active abduction. If intrinsic loads are too great with the introduction of active elevation, use axially loaded exercises as a transition to OKC(open kinetic chain) exercises. In these exercises, the patient applies a moderate weight through the upper extremity, as in the CKC exercises, but also slides the arm into elevation. Wall slides(as in the above pictures) and table slides are examples. Include trunk and hip motion with these exercises.
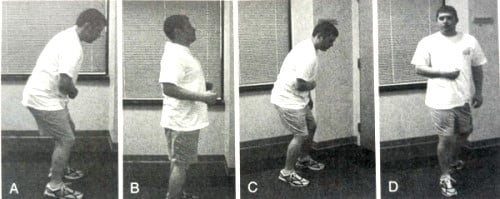
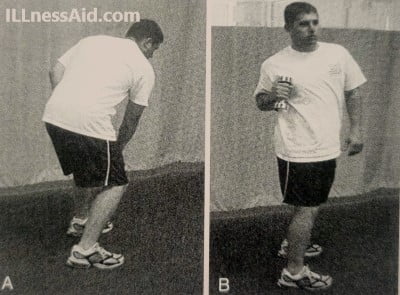
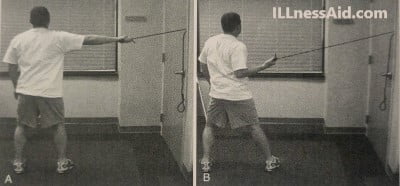
- “Open the chain” using a short lever, and transverse plane movements such as during the lawnmower exercise(as in the above pictures). The rotary motion helps facilitate scapular retraction and reduces the demand on the shoulder muscles.
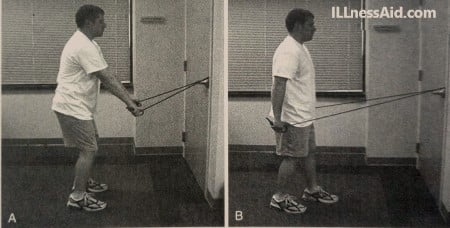
- Should begin tubing exercises using hip and trunk extension with retraction and also hip abduction and trunk flexion with retraction. You should use various angles of pull and planes of motion. De-emphasize upward pull until upper trapezius dominance eliminate.
- As scapulohumeral coupling and control achieve, dumbbell punches may introduce. Use complementary steps to incorporate the kinetic chain contribution and reciprocal motions. Change the height of punches while maintaining scapular control.
Functional Phase (6-10 Weeks)
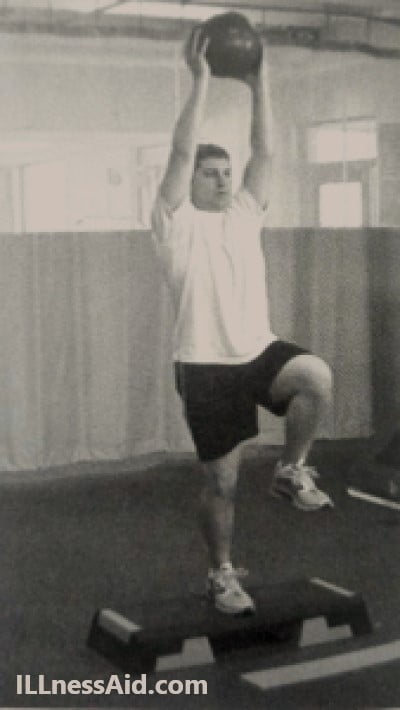
- When there is good scapular control and motion through the full range of shoulder elevation, should initiate plyometric exercises like medicine ball toss and catch.
- Continue to include kinetic chain activation. Move to various planes as there is improvement in scapular control.
- Slow, resisted, movements, such as the throwing motion, are helpful in promoting the kinetic chain stabilization while dynamically loading the scapular muscles.
- Overhead activities, in various planes, are advanced exercises that require good scapular control through a full and loaded Glenohumeral joint Range of motion
- Progressively add external resistance to earlier exercises. The volume of work becomes a progression, as do the difficulty of the exercise and the amount of resistance.
- Wobble boards, trampolines, and slide boards, which challenge lower extremity stability, also increase the load on the scapular musculature without sacrificing the functional movements.

Exercises are the solution of all problems
ILLnessAid
Thank you for reading this far, Today we talk about scapular dyskinesis, and we talk about rehabilitation programs also. If you have any doubts regarding this you can comment below or go on the contact us page.