The scaphoid fracture is the most common fracture in the carpal bones. Carpal fractures are often difficult to diagnose and treat. There are many complications including nonunion and malunion. Which changes wrist kinematics and can lead to pain, decrease in strength, decrease range of motion, and early radiocarpal arthrosis.
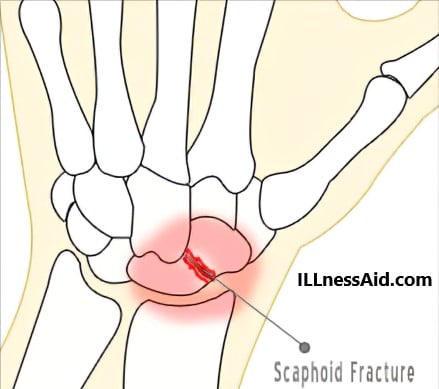
Scaphoid fractures are classified by the location of the fracture:
- Proximal Third
- Middle Third or Waist (This is the most common)
- Distal Third or Tuberosity (This is rare)
CAUSE AND SYMPTOMS
The scaphoid fracture usually happens during “hyperextension and radial flexion of the wrist“. It is most often in young active male patients. Patients usually have tenderness between the first and the third dorsal compartments (anatomic snuffbox). And less tenderness commonly on the distal scaphoid tuberosity volarly. Scaphoid fracture patients may have pain with compression of the thumb metacarpal.
EXAMINATION OF SCAPHOID FRACTURE
A scaphoid fracture is difficult to examine radiographically because of its oblique orientation in the wrist. Initial radiographs should include oblique, lateral, posteroanterior, and ulnar flexion. And an MRI is extremely sensitive in detecting this fracture as early as 2 days after injury. Now if an MRI is not available, Patients with snuffbox tenderness should immobilize for 10 to 14 days and then return for repeat radiographs. If you are not still diagnosed then do a bone scan.
Assessment for scaphoid fracture displacement is a key role in treatment. It is often assessed with a thin section(1mm) CT scan. Displacement defines as:
- More than 1 mm in the fracture gap
- An angle greater than 60 degrees of lateral scapholunate
- The angle of lateral radiolunate greater than 15 degrees
- The angle of the Intrascaphoid greater than 35 degrees
TREATMENT FOR SCAPHOID FRACTURE
Nondisplaced fractures can treat closed and always heal with thumb spica cast immobilization. Above or below elbow casting is still a controversial issue. We suggest 6 weeks of long arm thumb spica casting. You can confirm the union of scaphoids with a thin-section CT scan. For the surgical treatment these indications should be shown:
- Displaced scaphoid fracture
- Scaphoid nonunions show
- You do not treat your scaphoid fracture previously
- Nondisplaced fracture in which the prolonged immobilization would be intolerable
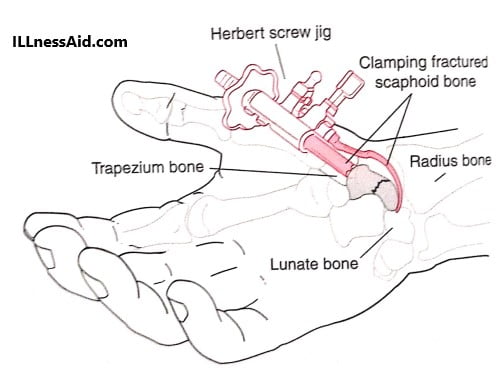
For displaced fractures, open reduction internal fixation is mandatory(ORIF). A recent meta-analysis reported that percutaneous fixation should result in 5 weeks earlier than cast treatment and return to the work 7 weeks earlier. Now let’s discuss rehabilitation programs for both Non displaced fracture and displaced fracture (treated with ORIF).
REHABILITATION PROGRAM
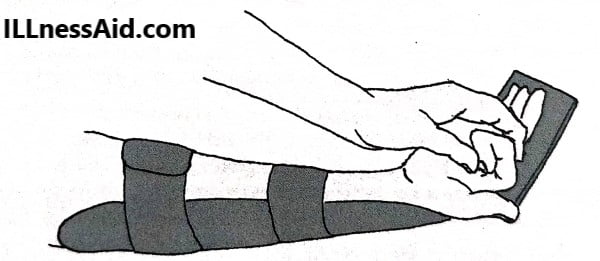
FOR FRACTURES TREATED CLOSED, TREATMENT IN THUMB SPICA CAST
0-6 Weeks
- Use a sugar-tong thumb spica cast
- Active shoulder range of motion
- Active second through fifth MCP/PIP/DIP joint Range of motion
6-12 Weeks (Bony Union)
- Non-tender to palpation, painless range of motion with cast-off
- Use short arm thumb spica cast
- Continue the shoulder and finger exercises
- Begin active elbow flexion/extension and forearm supination/pronation
12 Weeks
- CT scan is to confirm union. If show not united, continue short arm thumb spica cast
12-14 WEEKS
- Assuming union fracture at 12 weeks, removable thumb spica splint
- Start a home exercise program
- Should do active/gentle-assisted wrist flexion/extension range of motion
- Do active/gentle-assisted wrist radial/ulnar flexion range of motion
- Also, do active/gentle-assisted thumb MCP/IP joint range of motion
- Do active/gentle-assisted thenar cone exercise
14-18 Weeks
- Should Discontinue all splinting
- Formalized physical/occupational therapy
- Do active/aggressive-assisted wrist flexion/extension range of motion
- Should do active/aggressive-assisted wrist radial/ulnar flexion range of motion
- Do active/aggressive-assisted thumb MCP/IP joint range of motion
- Do active/aggressive-assisted thenar cone exercise
18 Weeks +
- Do grip strengthening, aggressive ROM
- Unrestricted activities

FOR SCAPHOID FRACTURE TREATED WITH ORIF
0-10 Days
- Use Elevate sugar-tong thumb spica splint, ice.
- Start shoulder range of motion
- MCP/PIP/DIP joint active range of motion exercises
10 Days-4 Weeks
- Suture removal
- Use a sugar-tong thumb spica cast (immobilizing elbow).
- Continue hand/shoulder range of motion
4-8 Weeks
- Use Short arm thumb spica cast
- Elbow active/assisted extension, flexion/supination/ pronation; continue fingers 2 through 5 active ROM and shoulder active range of motion
8 Weeks
- Should use CT scan to verify union of fracture
8-10 Weeks (Assuming Union)
- Should remove thumb spica splint
- Start a home exercise program
- Do Active/gentle-assisted wrist flexion and extension ROM
- Should do Active/gentle-assisted wrist radial/ulnar flexion ROM
- Do Active/gentle-assisted thumb MCP/IP joint ROM
- Should do Active/gentle-assisted thenar cone exercise
10-14 Weeks
- Should Discontinue all splinting
- Formalized physical/occupational therapy
- Should do active/aggressive-assisted wrist flexion/extension range of motion
- Do active/aggressive-assisted wrist radial/ulnar flexion range of motion
- Do Active/aggressive-assisted thumb MCP/IP joint range of motion
- Should do Active/aggressive-assisted thenar cone exercise
14 Weeks +
- Start Grip strengthening by using grip ball
- Aggressive range of motion
- Unrestricted activities
DO NOT IGNORE YOUR PAIN IT CAN LEAD TO BIG PROBLEM
ILLnessAid
Thank you for reading this far, today we talk about the scaphoid fracture. If you have any doubts regarding this then comment below or go on the contact us page.