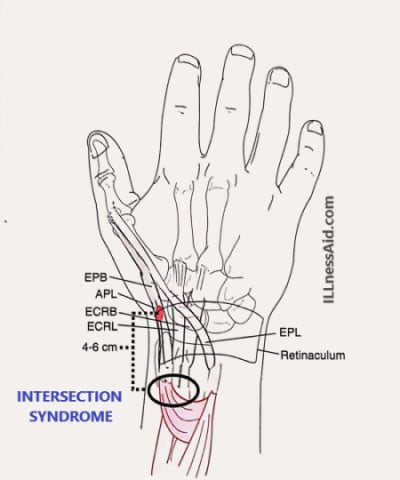
The “intersection” in this syndrome refers to the crossover site of the first and second dorsal compartment of the wrist. The first compartment consists of the abductor pollicis longus(APL) and Extensor pollicis brevis(EPB), and the second compartment consists of the extensor carpi radialis longus(ECRL) and extensor carpi radialis brevis(ECRB). These compartments traverse each other at a 60-degree angle. This condition area is noted:
- Around 4cm – 6cm proximal to the radial styloid
- Having pain,
- Swelling,
- Edema,
- Crepitance in patients
CAUSES OF INJURY
Intersection syndrome is due to overuse which means It occurs with repetition movement of wrist flexion and extension. Common sports for intersection syndrome are rowing, skiing, racquetball or tennis, weightlifting, and canoeing. Weightlifters who overuse radial extensors muscles of the wrist and perform excessive curling movements are vulnerable to intersection syndrome. In rowing athletes, many factors are the reasons for wrist injuries including wrong grip size, high winds, poor water, and poor shoulder(trunk stabilization techniques). And improper pull and throw using the elbow instead of the shoulder.
EXAMINATION FOR INTERSECTION SYNDROME
Making a definite examination in a patient with wrist pain is very challenging because of the proximity of the many structures (complex anatomy). Intersection syndrome is often misdiagnosed as “de Quervain tenosynovitis” because of the location. So let’s understand how can we examine accurately.
PHYSICAL EXAMINATION
- To examine the tenderness point of this syndrome, you should palpate the dorsum of the wrist. And three fingerbreadths proximal to the wrist joint( 4 to 6cm).
- Crepitation or Squeaking is also noted with active or passive movement that involves tendon
- Swelling is also visible in both compartments of muscles.
- Pain is present during wrist flexion and extension rather than on radial and ulnar deviation(as in de Quervain tenosynovitis).
- In the Finkelstein test, the pain will be exacerbated but it will be more proximal than de Quervain tenosynovitis.
RADIOGRAPHIC EXAMINATION
Plain radiographs of the wrist can use to rule out alignment problems but these are mostly normal in intersection syndrome. For persistent symptoms musculoskeletal ultrasound and MRI are useful. MRI helps to find tendon thickening, intrasubstance tendon signal, edema of muscle, and peritendinous edema. MRI images should include fluid-sensitive sequences.
Musculoskeletal ultrasound findings are the same tp the MRI for tendon thickening and peritendinous fluid. Ultrasound helps in easy comparison to the asymptomatic side. And It also helps by dynamic images to show friction between the compartments.
TREATMENT FOR INTERSECTION SYNDROME
In intersection syndrome, Conservative treatment is successful for 60% of patients. Conservative treatment includes the following:
- You can not do exacerbating activities like rowing
- You have to immobilize the thumb and wrist joint with a commercial thumb spica for 3 to 6 weeks. The splint should wear during the daytime and during sleep time also.
- Go to the cryo therapist and take cryotherapy several times a day
- Take NSAIDs with the recommendation of doctors
- Corticosteroid injections are also effective in patients whose pain is persisting despite the immobilization for 2 to 3 weeks and NSAIDs do not show effect.
- Gentle range of motion exercises of the wrist and hand should start, and the Wrist extensor strengthening exercise begins after the patient is asymptomatic for 2 to 3 weeks.
- You have to do exercise for strengthening the shoulder and trunk because it helps in correcting the mechanics of injury.
- You have to modify the training when activity is resumed like avoiding excessive weight curling or changing the grip in racquet sports
Now, When conservation treatment does not relieve the symptoms then surgery is reserved for those patients. So you should go to the doctor and consult about your problem. Now let’s talk about the “Rehabilitation phase after surgical decompression of intersection syndrome“:
REHABILITATION PHASE AFTER SURGICAL DECOMPRESSION
O-14 DAYS
- You have to keep the wrist in a neutral position within a surgical plaster splint
- Should encourage thumb, elbow, and digit motion as you are comfort
- Remove the sutures around 10-14 days (consult your doctor first) after surgery
2-4 WEEKS
- You have to maintain the presurgical splint until you can perform the activities of daily living(ADL) with small pain
- Active and active-assisted wrist extensor and flexion exercises should start
4-6 WEEKS
- Now, you begin the strengthening exercises
- You should do full activities at the end of the sixth week after surgery
- A splint can use as your need
- You should also follow the scar management technique

KNOWING THE TREATMENT DOES NOT MEANS YOU ARE DOCTOR OR THERAPIST
ILLnessAid
Thank you for reading this far, today we talk about intersection syndrome and how can we diagnose this. If you have any doubts regarding this, you can comment below or go on the contact us page.