Metacarpal neck fractures are the most common fractures in the hand. Fracture of the fifth metacarpal is most frequent and also known as “Boxer’s fracture“. It is known this name because the mechanism is a glancing punch that does not land on stronger 2nd and 3rd metacarpals.
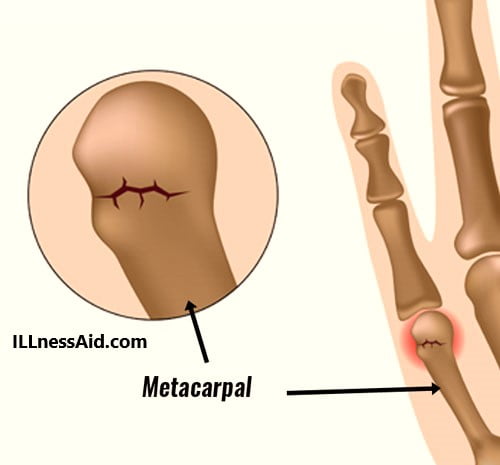
Generally, This fracture happens when you hit a punch on a wall or hard surface. It means that punching a solid surface with a closed fist can lead to a fracture. This fracture happens because its weakest point is the neck of the metacarpal bone.
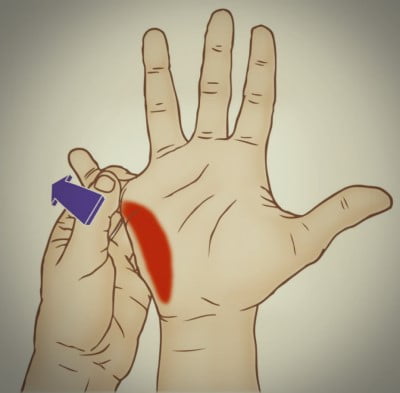
SYMPTOMS AND EXAMINATION
Patients usually have(around MCP joint):
- Pain
- Swelling
- Loss of motion
- The rotational deformity may present
- Popping sensations
- Discolor in skin
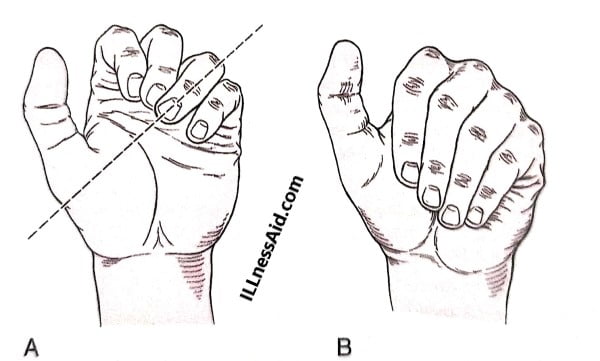
For a boxer’s fracture, A careful examination should perform to ensure that:
- There is no malrotation of the 5th finger when the patient makes a fist as in the picture below
- There is no Uncommon prominence of the distal fragment (palmary displaced)
- Should also see that no extensor lag of the involved finger
On the lateral radiograph, The angle of the metacarpal fracture is seen by drawing lines down the shafts of the metacarpal and measuring the angle(with a goniometer).
TREATMENT FOR BOXER’S FRACTURE
Treatment of the boxer’s fracture is based on the degree of angulation or displacement, as we measure on a true lateral radiograph of the hand. Metacarpal neck fractures are mostly impacted and angulated, with the fragment displacing palmarly and It is because of intrinsic muscle pull. Excessive angulation causes MCP joint knuckle loss and may cause the palmar metacarpal head prominent during work or activities.
Only 10 degrees of angulation can accept in 2nd and 3rd metacarpal neck fractures, Whereas up to 30 degrees in the 4th metacarpal and 40 degrees in the fifth metacarpal can accept. It is because of greater mobility in the 4th and 5th CMC joints.
- NOTE: Normal metacarpal neck angle is 15 degrees and a measured angle on the radiograph of 30 degrees is equal to 15 degrees.
- There is a report that says 30 degrees of MCP angulation results in a loss of 22%-23% of finger range of motion.
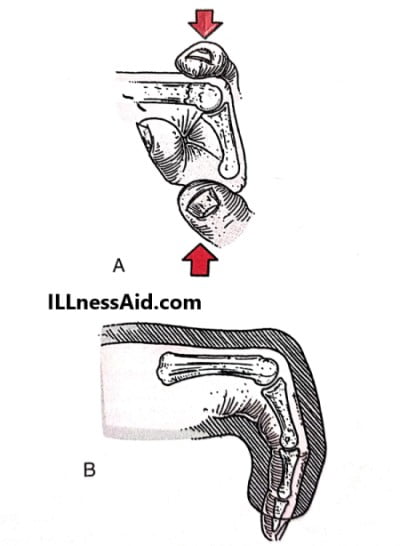
A closed reduction can attempt with wrist block anesthesia using a maneuver(credit to jahss) If displacement is unacceptable. In this, the proximal phalanx flexes to 90 degrees and use to apply direct force (dorsally) to the metacarpal head. Now hand will be splinted in an ulnar gutter splint for about 3 weeks with MCP joint at 80 degrees of flexion, DIP joint-free, and PIP joint straight.
- Rapid mobilization of the finger requires avoiding adhesions, scarring, and stiffness that is unrelated to the fracture itself. But rather to the tendency of an immobilized hand to quickly stiffen.
STATIUS MULLER TREATMENT
He treated around 35 patients with boxer’s fracture with an average fracture angulation of 39 degrees( range 15 to 70 degrees). Patients were treated with an ulnar gutter plaster cast for a 3 weeks period and then follow by mobilization. Or a pressure bandage for 1 week and then immediately mobilization within limits imposed by pain.
In both treatment processes, There is no statistical difference found with respect to ROM, satisfaction, return to work, hobby, and pain perception. But most clinics provide pressure bandage technique with good results for boxer’s fractures.
- NOTE: Boxer’s fractures can treat by simple methods and a great example is done by Bansal and Craigen. They treated 40 boxer’s fractures with casting and reduction. And also 40 cases with only taping and range of motion with instructions to return if a problem is experienced.
OPERATIVE TREATMENT
Operative treatment of boxer’s fractures indicates If the following occur:
- Alignment of fracture remains unacceptable
- Previously reduced fracture redisplacement occurs
- Malrotation of the finger present
Operative fixation generally involves percutaneous pinning of the fracture, But ORIF (open reduction internal fixation) may require. Fractures that treat operatively still require 3 weeks of protective splinting and range of motion exercises.
EXERCISES FOR BOXER’S FRACTURE
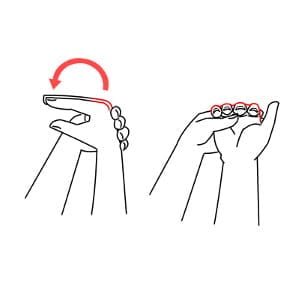
LITTLE FINGER EXTENSION
- For this, you need to put your little finger in a neutral position.
- Then with your other hand, bend your little finger backward, until you feel a gentle stretch.
- Hold the extended position for 5-10 seconds and then repeat the process.
FINGER FLEXION
- For this, start with all your fingers in a straight position.
- Then bend them forward at the knuckles by using your other hand.
- Hold them in the flex position for about 10 seconds and then repeat it 5-10 times.
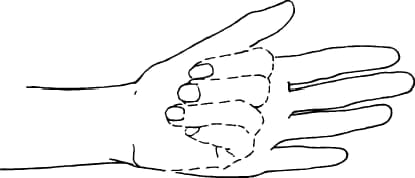
HOOK FIST
- Start with your fingers straight.
- Now, bend your fingers forwards as in the above exercise, but this time, keep your knuckles straight.
- In this, you need to bend both the interphalangeal joints of the fingers.
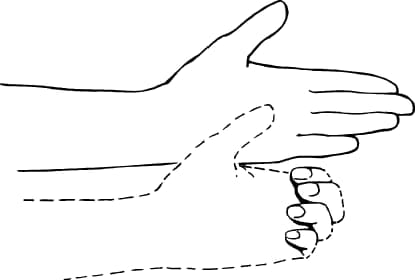
STRAIGHT FIST
- Starting position will remain the same as above.
- For this, flex your fingers by your knuckles and by the proximal interphalangeal joint.
- Remember to keep your distal interphalangeal joint in extension.
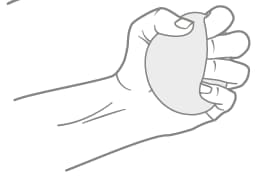
BALL GRIP
- For this, you need to take a softball in your hand.
- Bend your fingers forwards in order to grip the ball with your hand.
- Try to hold the ball in your hand for a few seconds and then repeat several times.
FULL FIST
- Start with your fingers straight.
- For this exercise, you need to bend your fingers forward by your knuckles as well as your interphalangeal joints (both proximal and distal).
- Hold this position for at least 10 seconds and then repeat.

Make sure where you are punching
ILLnessAid
Thank you for reading this far, today we talk about a boxer’s fracture and its treatment. If you have any doubt regarding this you can comment below or go on the contact us page.
Your blog post had me hooked from the first sentence.
Thank you, Brice Kian Billy Flowers, for your kind words about the blog post on Boxer’s Fracture. It’s great to hear that the first sentence managed to capture your interest. Providing an engaging introduction is crucial in capturing readers’ attention and setting the tone for the rest of the article. Feel free to let us know if you have any specific questions or if there’s anything else you’d like to discuss regarding the topic.