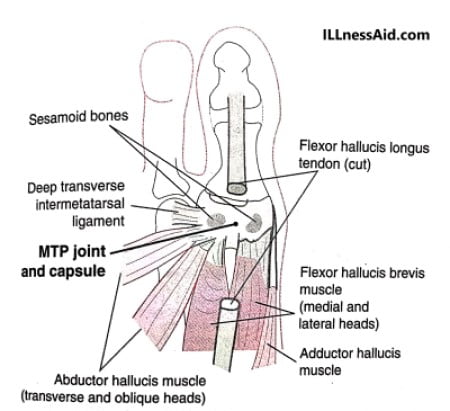
The turf toe describes a range of injuries to the capsuloligamentous complex of the first MTP (metatarsophalangeal) joint. ROM of the MTP joint is variable and power to move the joint is provided by both intrinsic and extrinsic muscles group. Two sesamoid bones – medial (tibial) sesamoid and lateral (fibular) sesamoid provide mechanical advantage to the intrinsic plantar flexors by increasing the distance between the empirical center of joint rotation and the respective tendons.
As pictured below, The sesamoid complex is attached with facets on the plantar aspect of the first metatarsal head and is stabilized by a plantar capsule. And a ridge on the metatarsal head that separates the two sesamoids.
CAUSES OF TURF TOE
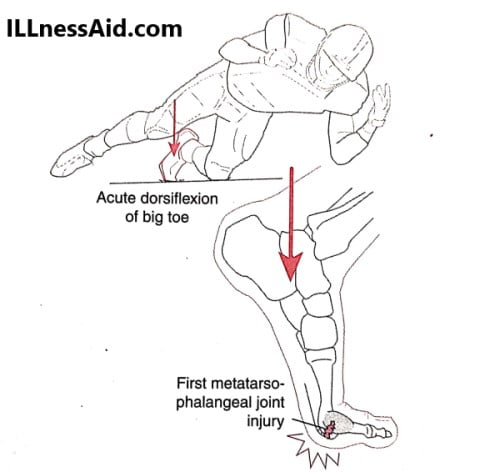
Forced dorsiflexion of the MTP joint is the mechanism of the turf toe. The typical football-associated injury occurs when a player firmly plants his forefoot then is struck from behind. The continued forward motion of the leg over the fixed forefoot produces hyperdorsiflexion of the first MTP joint and increased tension on the capsule. These forces may continue and produce a dorsal impaction Injury to the cartilage and bone of the head (metatarsal).
The extreme motion required to produce an injury is more likely to occur in a flexible shoe as opposed to a relatively stiff-soled shoe. The playing surface has been indicated as an associated factor. The hard playing surface of an artificial turf field may result in an increased incidence of first MTP joint sprain and the term is “Turf Toe“. A chronic, cumulative mechanism is associated with similar risk factors. Turf toe injury mechanism is by no means specific.
SIGNS AND SYMPTOMS
Turf Toe is associated with:
- Acute localized pain
- Swelling
- Ecchymosis
- Guarding
- Increasing degrees of swelling, pain, and loss of joint motion as the severity of the injury increases
- An antalgic gait and tendency to avoid loading may be present
EVALUATION OF TURF TOE
Standard radiographic evaluation of turf toe includes AP and lateral views of the weight-bearing foot and a sesamoid projection. Diagnosis is confirmed on the MRI when capsular tears and associated edema are confirmed. We can use a Bone scan, CT, and MRI used to rule out the problem.
For those patients who show turf toe, We can identify by physical examination like:
- First MTP joint swelling
- Plantar tenderness at the MTP joint
- Ecchymosis adjacent to an area of the capsular injury
- Pain with passive MTP joint dorsiflexion
- Pain with joint loading
- Decreased dorsiflexion of the MTP joint
A typical finding in patients with turf toe injuries from a radiographic examination include:
- Soft tissue swelling
- Small periarticular bony avulsions
- Intra-articular loose bodies
- Diastasis of bipartite sesamoid
- Sesamoid fracture
- Migration of the sesamoids
TREATMENT FOR TURF TOE
Acute injuries can treat with the RICE (rice, ice, compression, elevation) method followed by a gentle ROM program and protected weight-bearing. Taping is not good for an acute injury because it may compromise circulation. By using a short leg cast or walking boot we can protect the hallux from extension at the MTP joint and allow the athlete to bear weight. Gentle ROM exercises can begin as early as 3 to 5 days after injury if symptoms allow. Low impact exercises can attempt with toe protected with boot or toe spica taping. But explosive, push-off activities should not try until low-impact exercises are pain-free.
Chronic injuries treat with the ROM program and protected weight-bearing. The hallux MTP joint can support by a variety of methods. walking cast, rigid shoe modification, stiff-soled shoes, and various taping methods. Joints also protect by reducing activity levels, increasing rest intervals. NSAIDs and ICE help to reduce inflammation. Intra-articular steroids are of no benefits and may be detrimental to the joint.
Operative treatment is rare for isolated turf toe. Occasionally, an associated condition identifies in which surgery becomes a treatment. Prevention of turf toe includes the use of supportive footwear and firm inserts and avoidance of hard playing areas or surfaces.
REHABILITATION TREATMENT PLAN FOR TURF TOE
PHASE I: ACUTE PHASE (Days 0-5)
- Rest, ice, ice bath, whirlpool bath, contrast bath, and ultrasound for pain, inflammation, and joint stiffness.
- joint Mobilization should follow a gentle, passive, and active range of motion.
- Do isometrics around the metatarsophalangeal joint as pain allows.
- Cross-training activities, like water activities, and cycling for aerobic fitness.
- Use protective taping and shoe modifications for continued weightbearing activities and work.
Phase 2: Subacute Phase-Weeks 1-6
- Modalities to joint stiffness and decrease inflammation.
- Emphasis on increasing flexibility and Range of motion, with both active and passive methods and joint mobilization.
- Progressive strengthening
- Towel scrunches
- Toe pick-up activities.
- Manual resistive hallux MTP dorsiflexion and planterflexion.
- Do seated toe and ankle dorsiflexion with progression to standing.
- Should do toe dorsiflexion in sitting position with progression to standing.
- Seated supination-pronation with progression to standing
- Balance activities, with the progression of moderate to difficult to include biomechanical ankle platform system (BAPS)
- Cross-training activities (slide board, cycling, water running) to maintain aerobic fitness.
Phase 3: Return-to-Sport Phase-Week 7
- Continued use of protective inserts or taping.
- Continued ROM and strength exercises.
- Should running, to progress within limits of a pain-free schedule.
- Monitored plyometric and cutting program, with the progression of difficulty.
- Care should be taken to avoid reinjury during these activities and work

BE TRUTH TO YOUR PAIN
ILLnessAid
Thank you for reading this far, today we talk turf toe and treatment about it. If you have any doubts regarding this, you can comment below or go on the contact us page.